As the world debates the origin of SARS-COV-2, most assume the SARS outbreak of 2003 was a natural event. But revisiting the evidence I found parallels, direct linkages and many unresolved questions.
To understand the origin of SARS-CoV-2 it’s illuminating to revisit the history of the first SARS outbreak and the subsequent investigation of its origin. SARS is assumed to be the result of a natural zoonosis by most scientists – including many who are open to an artificial origin of SARS-CoV-2. But the basis for this assumption may be unsound. There are many parallels between the two viruses both at the molecular level, and also in the epidemiology, pandemic management and origins tracing. Many of the same individuals and institutions play key roles in both. It may be that these outbreaks aren’t independent events, but the result of a long-term research program.
Due to the health crisis caused by SARS-CoV-2, the creation of a new vaccine platform based on mRNA was implemented. Globally, around 13.32 billion COVID-19 vaccine doses of diverse platforms have been given, and up to this date, 69.7% of the total population received at least one injection of a COVID-19 vaccine. Although these vaccines prevent hospitalization and severe forms of the disease, increasing evidence has shown they do not produce sterilizing immunity, allowing people to suffer frequent re-infections. Recent research has also raised concerns that mRNA vaccines could induce immune tolerance, which, added to that caused by the virus itself, could complicate the clinical course of a COVID-19 infection. Furthermore, recent investigations have found high IgG4 levels in people who were administered two or more injections of mRNA vaccines. It has been suggested that an increase in IgG4 levels could have a protecting role by preventing immune over-activation, similar to that occurring during successful allergen-specific immunotherapy by inhibiting IgE-induced effects. Altogether, evidence suggests that the reported increase in the IgG4 levels detected after repeated vaccination with the mRNA vaccines is not a protective mechanism; rather, it may be a part of the immune tolerance mechanism to the spike protein that could promote unopposed SARS-CoV2 infection and replication by suppressing natural antiviral responses. IgG4-induced suppression of the immune system due to repeated vaccination can also cause autoimmune diseases, promotes cancer growth, and autoimmune myocarditis in susceptible individuals.
TL:DR – Long covid has no link to prior COVID19, instead, initial symptom severity (of whatever virus you get), loneliness and poor physical activity are linked to the “post covid conditions”
I have served on or chaired two dozen data safety monitoring boards for randomized trials of novel experimental drugs or devices. I can tell you firsthand for COVID-19 vaccines, a 30-day regulatory window after injection is fair game for attribution of adverse events to the product when the special complications of interest are known to be caused by the mRNA induced Wuhan Spike protein.
Jabagi et al., NEJM, reported from the French National Health Data System linked to the national COVID-19 vaccination database disclosing cardiovascular events after mRNA BA4/BA5 bivalent boosters. All persons who were 50 years of age or older and who had received a booster dose between October 6 and November 9, 2022, were included in the study. The composite of ischemic/hemorrhagic stroke, myocardial infarction, or pulmonary occurred in 335 unfortunate individuals.
Public health agencies should be held to a high standard, yet they are getting away with spreading false information and accusing others who have posted factual information, of doing the same.
“It’s like a horror movie I’m being forced to watch and I can’t close my eyes,” one senior FDA official said. “People are getting bad advice and we can’t say anything.”
It’s a shame that the agencies tasked with protecting us may be doing the exact opposite. It’s nearly impossible to rely on them for accurate information, guidance and data when it comes to all things health.
If physicians and public health officials in the US remain silent and fail to admit past mistakes, harmful policies will persist or resurface in the next pandemic. Why wouldn’t they? Without us defining what went wrong or creating an ethical framework to prevent the same mistakes, why would they stop?
Proof that the miscarriage rate after the COVID vaccines is far higher than the real background rate and how the pharma corporations hide it
This story is not going away, however much the pharma companies and their vaccination-in-pregnancy foot soldiers want it to. The recent revelations of the #Placentagate scandal has brought it to a head, and we are going to keep gnawing away.
8/8 monovalent vaccines sourced from a single case from a single lot of Pfizer monovalent vaccines all fail the EMA specification of 3030:1 RNA:DNA (330ng/mg DNA/RNA). They are over the limit by an order of magnitude (18-70 fold). The DNA contamination is very consistent and the vial to vial ratio of RNA:DNA is very consistent within the same lot of monovalent vaccines. Further sequencing is underway to evaluate the 72bp heteroplasmic indel in the SV40 promoter of the vector. This was detected in the Pfizer bivalent vaccines.
“Something’s going on with our workforce that we’ve never seen before. And it’s gone so far above trend — it’s a health concern.”
The 2022 absence rate “makes absolutely no sense,” exclaimed former Blackrock portfolio manager Edward Dowd. “Something’s going on with our workforce that we’ve never seen before. And it’s gone so far above trend — it’s a health concern.”
“Absences are defined as instances when persons who usually work 35 or more hours a week worked less than 35 hours during the reference week for one of the following reasons: Own illness, injury, or medical problems; child-care problems; other family or personal obligations; civic or military duty; and maternity or paternity leave. Excluded are situations in which work was missed due to vacation or personal days, holiday, labor disputes, and other reasons. For multiple jobholders, absence data refer only to work missed at their main jobs. The absence rate is the ratio of workers with absences to total full-time wage and salary employment,” explained Mr. Dowd on his website.
He noted, “In relative terms, the deviation from trend in 2022, for the total (men+women) full-time workers was about 70%.”
“And that number [absence rates] went up three standard deviations off of trend (2003 to 2019)” in 2020, Mr. Dowd explained. In geek-speak, the chance of something three standard deviations above the mean is 0.3 percent.
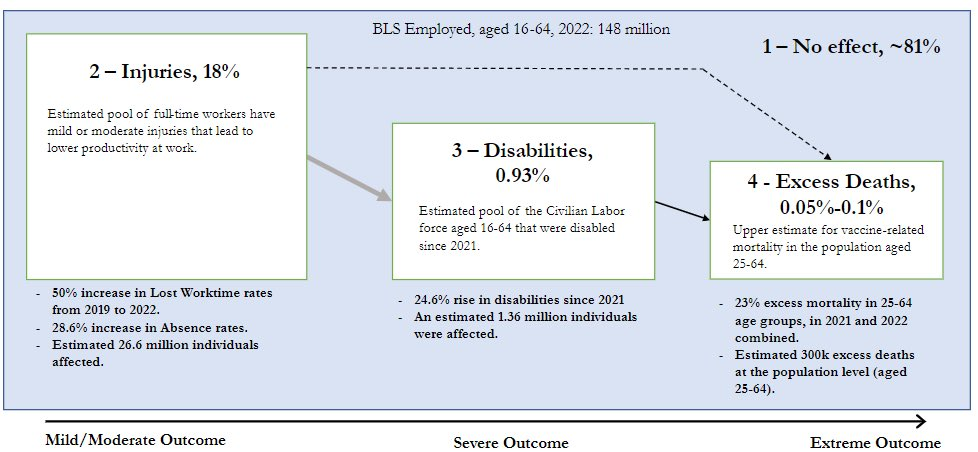
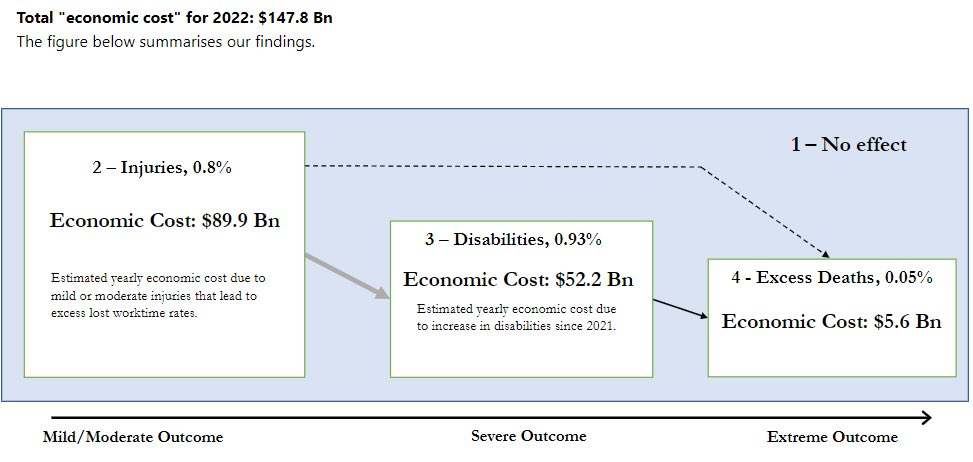
A new report estimates that 26.6 million people were injured, 1.36 million disabled, and 300,000 excess deaths can be attributed to COVID-19 vaccine damages in 2022 alone, which cost the economy nearly $150 billion.
Research firm Phinance Technologies, founded and operated by former Blackrock portfolio manager Ed Dowd, Yuri Nunes (PhD Physics, MSc Mathematics) and Carlos Alegria (PhD Physics, Finance), split the impact of the vaccines into four broad categories to estimate the human costs associated with the Covid-19 vaccine; no effect or asymptomatic, those who sustained injuries (mild-to-moderate outcome), those who became disabled (severe outcome), and death (extreme outcome). Data on vaccine disabilities and injuries comes directly from the Bureau of Labor Statistics (BLS), while the excess death figures are derived from official figures on deaths in the US via two different methods (methodology here).
It’s important to note that people in one category (injured, for example) can move into latter categories of severity – which this analysis does not take into consideration.
“We need to remember that not only are these groupings an attempt to characterize different levels of damage from the inoculations, they are not static and could interact with each other,” reads the report. “For instance, there might be individuals who had no visible effects after vaccination but nonetheless could still be impacted.”
“Individuals with mild injuries from the inoculations could, over time, develop severe injuries to the extent of being disabled, or an extreme outcome such as death.”
The analysis of disabilities is split into 5 parts that can be read independently but are related and complement each other. Each section is written in a different web page within which at the top the user can find the links to navigate to the other sections. The 5 parts are:
Part 1 – Overview of the Data. Go to Part 1 This part provides the overall description of the data and shows the historical time series of disability rates for different population cohorts and age groups. It allows us to put in perspective the changes in disability rates, that started in 2021.
Part 2 – Rise in disabilities from 2021. Go to Part 2 This part provides a detailed examination of the changes in disabilities that ocurred from early 2021, which coincided with the vaccine rollouts.
Part 3 – Relationship with Vaccine uptake. Go to Part 3 This part analyses the relationship between the rise in disabilities with the Covid-19 vaccine rollout.
Part 4 – Relationship with Excess Deaths. Go to Part 4 This part investigates the relationship between excess mortality and the rise in disabilities that ocurred since early 2021. It also provides us with an estimate of how many disabilities occurred for each excess death, during the period.
Part 5 – Relationship with SAEs in mRNA clinical trials Go to Part 5 This part investigates the relationship between Serious Adverse Events (SAEs) from the mRNA clinical trials with the rise in disabilities that ocurred since early 2021.
Part 6 – Relationship with Severe AEs in Pfizer vaccine clinical trial Go to Part 6 This part investigates the relationship between Adverse Events (AEs) and Severe Adverse Events (Sev AEs) from the Pfizer clinical trial with the rise in disabilities that ocurred since early 2021.
Our economic damage estimates are what we can measure. The knock effects such as lost productivity due to a worker being present but working at say 50%-75% of capacity is missed plus burn out from those picking up slack. Also supply chain delays are not captured etc and etc.…
This confirms that the TGA knew back in Jan 2021 that the lipid nanoparticles (and the mRNA) didn’t stay in the injection site, but spread throughout the entire body including the brain, the liver and ovaries.
Readers of ABN have known this for a long time. Similar information came from Japan some time ago and many researchers have provided this information in other ways. Still, this release from Australia is being recognized more readily in mainstream venues. Is your crazy sister going to believe it? Maybe not quite yet but we are getting closer. ABN