Abrien Aguirre: Covid in the park interview
This is an interesting interview. At 47:00 Aguirre outlines how and why the PCR test is bogus and how the nursing facilities were falsely changing billing codes to reap more federal covid money. ABN
Do your best. Speak the truth.

Abrien Aguirre: Covid in the park interview
This is an interesting interview. At 47:00 Aguirre outlines how and why the PCR test is bogus and how the nursing facilities were falsely changing billing codes to reap more federal covid money. ABN
The recent emergence of multiple SARS-CoV-2 variants has caused considerable concern due to reduced vaccine efficacy and escape from neutralizing antibody therapeutics. It is therefore paramount to develop therapeutic strategies that inhibit all known and future SARS-CoV-2 variants. Here we report that all SARS-CoV-2 variants analyzed, including variants of concern (VOC) Alpha, Beta, Gamma, and Delta, exhibit enhanced binding affinity to clinical grade and phase 2 tested recombinant human soluble ACE2 (APN01). Importantly, soluble ACE2 neutralized infection of VeroE6 cells and human lung epithelial cells by multiple VOC strains with markedly enhanced potency when compared to reference SARS-CoV-2 isolates. Effective inhibition of infections with SARS-CoV-2 variants was validated and confirmed in two independent laboratories. These data show that SARS-CoV-2 variants that have emerged around the world, including current VOC and several variants of interest, can be inhibited by soluble ACE2, providing proof of principle of a pan-SARS-CoV-2 therapeutic.
Clinical grade ACE2 as a universal agent to block SARS-CoV-2 variants
“I feel like I’m being treated unequally,” Aaron Kheriaty, professor of psychiatry and human behavior at the University of California, Irvine, said, SBG reported. “If my immunity is as good, indeed, very likely better, than that conferred by the vaccine, there doesn’t seem to be any rational basis for discriminating against my form of immunity and requiring me to get a different form of immunity.”
“It violates medical ethics to expose someone to this risk when they have robust, durable immunity that actually neutralizes SARS-CoV-2 upon exposure,” the faculty members wrote.
link
The safety signal analysis employed by the CDC, VSD, and associated regulatory agencies uses methods that are not simply ill-suited to the task, but mask substantial indications that large numbers of people are being injured, often seriously, or even killed by the COVID-19 vaccines currently in use. The inequivalent definitions used in mortality calculations results in inexcusably rigged risk-benefit analyses, and the lack of investigation into causes of mortality (both for the COVID-19 disease and also for the COVID-19 vaccines) stands out as historically monumental malpractice and dereliction of duty. The mass vaccination program should be halted while true risk-benefits of the vaccines are assessed, and regulatory agencies fully investigated for conflicts of interest and intention to defraud the public of its opportunity for informed consent.
Defining Away Vaccine Safety Signals, Part 3
This linked article is by Matthew Crawford. His work is essential to understanding the sleight-of-hand employed by the CDC and other agencies. I highly recommend more of us read what he is saying. ABN
Researchers discovered an enzyme that is genetically related to a key enzyme in snake venom and was found in COVID-19 fatalities in doses 20 times the safe amount.
link
There was no reduction in per-population daily mortality, hospital bed, ICU bed, or ventilator occupancy of COVID-19-positive patients attributable to the implementation of a mask-wearing mandate.
link
A new study of a series of cases in the Journal of Neurology examines possible links between Pfizer and Moderna vaccines, and acute Central Nervous System (CNS) demyelination, including Multiple Sclerosis (MS).
Demyelinating diseases damage the protective covering surrounding nerve fibers in the brain, optic nerves and spinal cord, causing neurological problems.
In the study, four patients had the Pfizer vaccine and three had the Moderna vaccine. Within 21 days of the first or second dose, the patients developed active CNS demyelination of the optic nerve, brain, and/or spinal cord leading to “visual loss, dysmetria, gait instability, paresthesias, sphincter disturbance, and limb weakness.”
link
ISSUED: September 3, 2021
The Texas Medical Board (TMB) and Texas State Board of Pharmacy (TSBP) do not endorse or prohibit any particular prescribed drugs or treatment for COVID-19 that meet the standard of care. Drugs are permitted to be prescribed off-label. It is the professional judgement of each physician to write their prescriptions while meeting all applicable federal and state statutes and rules. Similarly, each pharmacist must use their professional judgement in dispensing valid prescriptions while meeting all applicable federal and state statutes and rules.
link
Pockets of sanity forming inside USA. Very happy to see this emphasis on normal clinical practice. Doctors normally figure out how to treat new diseases starting at the individual patient-doctor level. At the same time, doctors talk to each other and share what works, what doses, when to give, etc. From there, good protocols can be established globally as has been done with HCQ, IVM, budesonide, and many other medications. Banning good treatments and mandating harmful treatments while censoring doctors and interfering with doctor-patient relations is not good science. It is a species of totalitarianism driven by immoral and perverse urges. ABN
Over the past decade, the global scientific community have begun to recognize the unmatched value of an extraordinary drug, ivermectin, that originates from a single microbe unearthed from soil in Japan. Work on ivermectin has seen its discoverer, Satoshi Ōmura, of Tokyo’s prestigious Kitasato Institute, receive the 2014 Gairdner Global Health Award and the 2015 Nobel Prize in Physiology or Medicine, which he shared with a collaborating partner in the discovery and development of the drug, William Campbell of Merck & Co. Incorporated. Today, ivermectin is continuing to surprise and excite scientists, offering more and more promise to help improve global public health by treating a diverse range of diseases, with its unexpected potential as an antibacterial, antiviral and anti-cancer agent being particularly extraordinary.
link
Just give everybody a kit with IVM and other meds to be used the moment they detect signs of covid. Teach doctors how to tailor doses and medications. Encourage doctors to do that. ABN
At some point, when the potential for conflicts of interest are high and the point of failure is fundamental to the task of those doing the job, incompetence should no longer be differentiated from criminal intent. Mathematicians and statisticians worthy of the title do not miss the kind of scale invariance or mean-reversion we see embedded in the PRR—particularly not when working in a dedicated group on a serious problem. There is a pride among geeks in identifying subtle mathematical or logical flaws in a system, and this is not subtle at all. Given that even psychologists have a need to pay attention to scale invariance, this is not an easily excused mistake. In fact, a computational check of the PRR function against past data likely would have clued in a middling programmer without the fundamental mathematical training. And we’re not done, yet…
…Calling this a safety system is decidedly unsafe. Even worse—given that numerous academics, including statisticians, reviewed this document, it is hard to believe that the scale invariance embedded in the definition of PRR, or the logic that includes meeting multiple criteria at the same time, went unnoticed. It certainly appears that the CDC’s goal was to establish an illusion of safety, and a reason to ignore the true signs of danger. At best, they unfathomably hired nobody whose job it was to remain independently-minded who could clue them in?
If my understanding of this situation is correct, the mass vaccination program should be immediately halted until the safety data is gathered, cleaned, and examined. We cannot tolerate a misleading statement of “vaccines are safe and effective” in the face of regulatory agencies defining away the responsibility of performing the risk analysis needed to verify safety. The CDC leadership should be immediately replaced and investigated, and independent analysts should reformulate the task of tracking vaccine safety results.
Defining Away Vaccine Safety Signals
Scientists and mathematicians, please read this paper. This is an intellectual smoking gun! Ordinary readers, it is not hard to follow this analysis. Well worth reading. Here is Crawford’s spicy rebuttal to critics: Defining Away Vaccine Safety Signals Part 2. ABN
It’s incredible to watch experts & politicians ignore this because it’s inconvenient for them

Originally tweeted by IM (@ianmSC) on September 5, 2021.
Israel was the first country to achieve large scale vaccinations of citizens over 40
It was assumed that the pandemic was over for them
Cases have grown again with the Delta variant
Do the vaccines work?
Let’s find out!
1
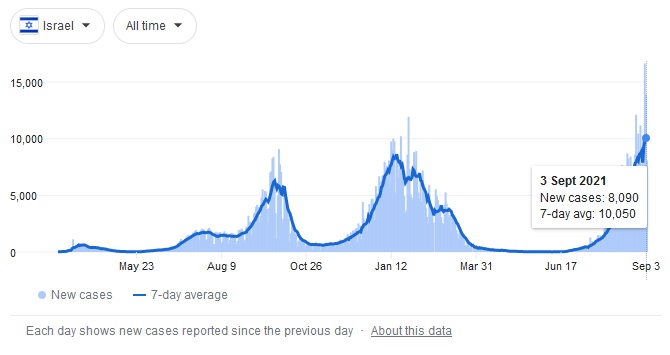
First off, you’re only as good as your data set
I’m working off of @yuvharpaz‘s data which is linked below
Thanks to @RanIsraeli for the heads up
[ABN: Lacking for me in this worthy analysis is death by vaccine. This number should be added to death for vaccinated who get covid. Even in Israel we do not seem to have good figures for vaccine mortality. Steve Kirsch has put the number as high as 150K in USA. ABN]
Continue reading “Pfizer Vaccine Effectiveness in Israel Deep Dive🚨”
As of September 1, only those who received 3 doses are considered “vaccinated”.
Health officials continue to move the goal posts. When will it finally be enough?



They have also stated their vaccine passports now expire 6 months after the 2nd Pfizer dose. That means you need booster shots to keep the vaccine passport valid.
Meanwhile, Israeli Health officials indicated that 90% of COVID-19 hospitalizations are fully vaccinated.
Originally tweeted by Dr. Simone Gold (@drsimonegold) on September 5, 2021.
