Matt Nespoli, Dad Presents Podcast, asked what do we anticipate for kids 20 years down the road after taking them? I unpack this specifically sub-clinical myocarditis where the kids do not feel the heart damage in their bodies. I cite Schauer, Baumeier, Mansanguan et al, 2021-22
Pfizer and Moderna mRNA COVID-19 vaccines were associated with an excess risk of serious adverse events of special interest of 10.1 and 15.1 per 10,000 vaccinated over placebo baselines of 17.6 and 42.2 (95 % CI −0.4 to 20.6 and −3.6 to 33.8), respectively. Combined, the mRNA vaccines were associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated (95 % CI 2.1 to 22.9); risk ratio 1.43 (95 % CI 1.07 to 1.92). The Pfizer trial exhibited a 36 % higher risk of serious adverse events in the vaccine group; risk difference 18.0 per 10,000 vaccinated (95 % CI 1.2 to 34.9); risk ratio 1.36 (95 % CI 1.02 to 1.83). The Moderna trial exhibited a 6 % higher risk of serious adverse events in the vaccine group: risk difference 7.1 per 10,000 (95 % CI –23.2 to 37.4); risk ratio 1.06 (95 % CI 0.84 to 1.33). Combined, there was a 16 % higher risk of serious adverse events in mRNA vaccine recipients: risk difference 13.2 (95 % CI −3.2 to 29.6); risk ratio 1.16 (95 % CI 0.97 to 1.39).
Discussion
The excess risk of serious adverse events found in our study points to the need for formal harm-benefit analyses, particularly those that are stratified according to risk of serious COVID-19 outcomes. These analyses will require public release of participant level datasets.
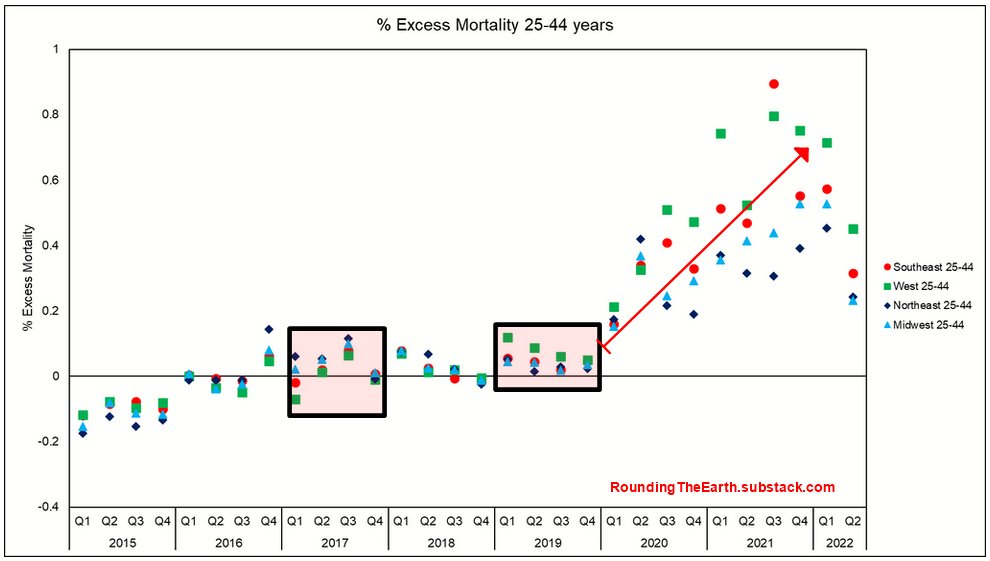
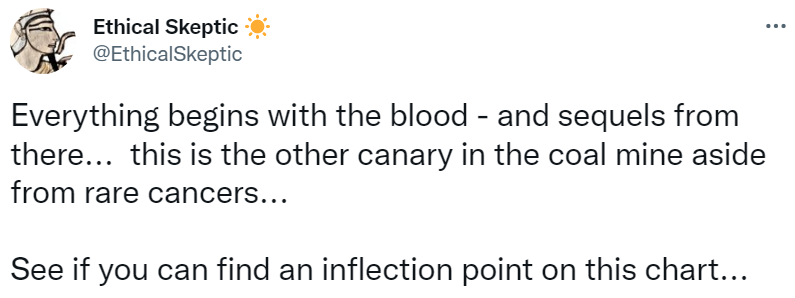
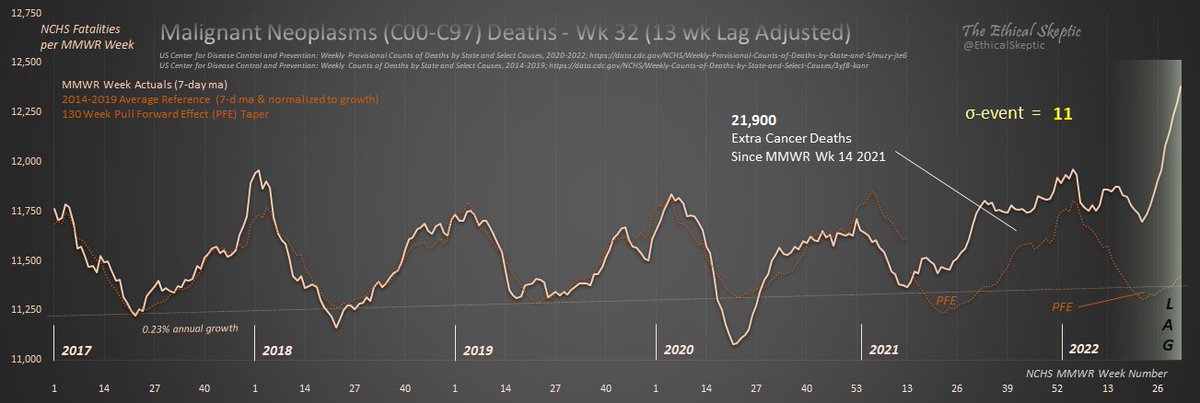
Seven of the major eleven International Classification of Diseases codes tracked by the US National Center for Health Statistics exhibit stark increase trends beginning in the first week of April 2021 – featuring exceptional growth more robust than during even the Covid-19 pandemic time frame. This date of inception is no coincidence, in that it also happens to coincide with a key inflection point regarding a specific body-system intervention in most of the US population. These seven pronounced increases in mortality alarmingly persist even now.
The following work is the result of thousands of hours of dynamic data tracking and research on the part of its author. The reader should anticipate herein, a journey which will take them through the methods and metrics which serve to identify this problem, along with a deductive assessment of the candidate causal mechanisms behind it. Alternatives as to cause which include one mechanism in particular, that is embargoed from being allowed as an explanation, nor even mere mention in some forums.
At the end of this process, we will be left with one inescapable conclusion. One which threatens the very fabric and future of health policy in the US for decades to come.
This article is a must-read. It is short and very clear. Click on the graphs because they are important for full understanding. In the above excerpt, “a specific body-system intervention in most of the US population” means mass covid vaccinations, as does “\/” elsewhere in this essay. TES could be wrong, but I doubt it. The CDC and NIH are absolutely morally obligated to explain these findings and/or openly accept them and resign en masse. ABN
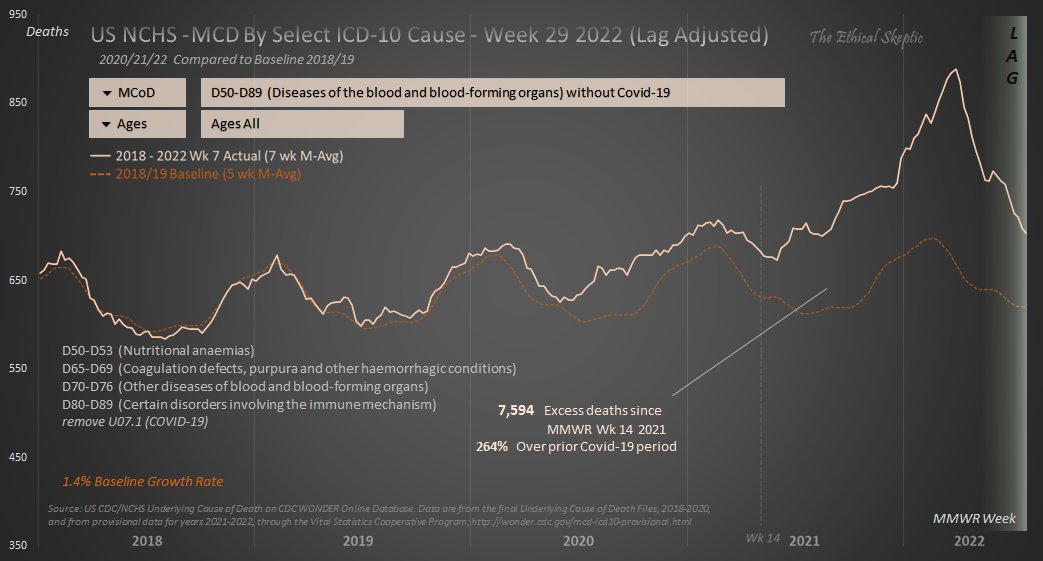
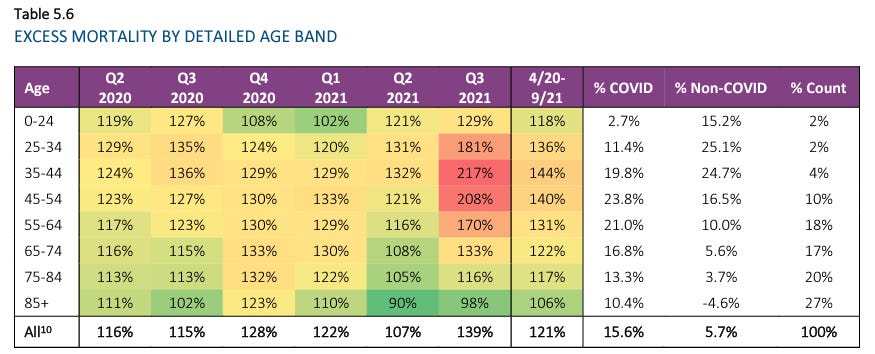
Excess mortality in Germany 2020–2022 is a preprint by Christof Kuhbandner (a psychologist at Regensburg) and Matthias Reitzner (a statistician at Osnabrück) that applies sophisticated actuarial analysis to the publicly available all-cause mortality data provided by the German government. It turns out that when you account for historical mortality trends, the virus no longer looks so dangerous, and the vaccines no longer look so great.
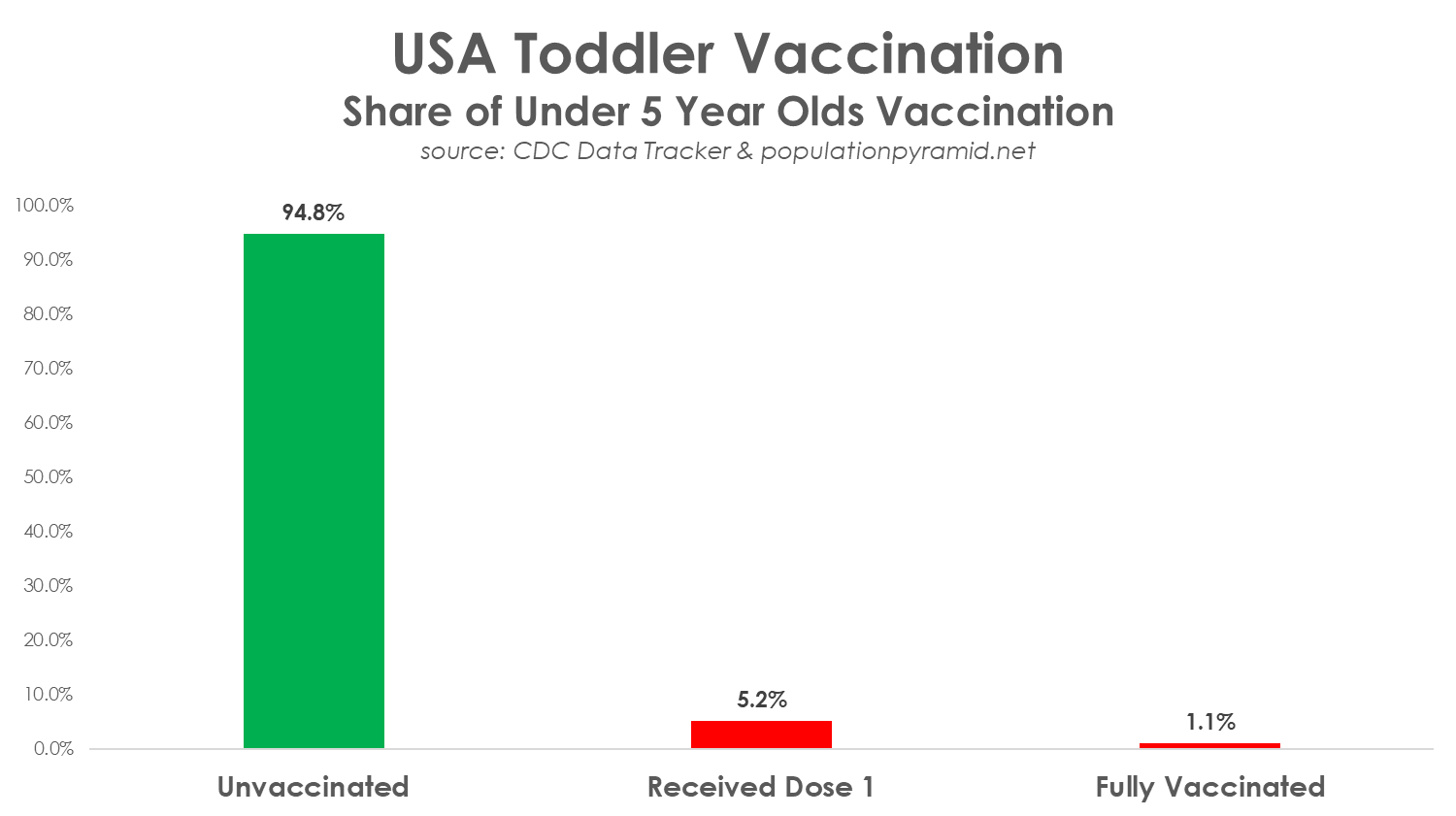
This figure may be one of the best indicators of the public’s understanding of vaccines and possibly all things covid. It is also an indicator of how badly the public perceives the federal government, health authorities, and covid “health” policies. This graph may probably also indicates the degree to which mainstream public polls are skewing the results of virtually all their polls—“nudging” the public to believe and act as Biden’s handlers want us the believe and act. ABN
Here is a quick summary of some of the things they said:
They are afraid to come out publicly due to intimidation tactics such as loss of job and/or license to practice medicine.
Unvaccinated healthcare workers are extremely upset with the medical community. They feel they have been treated unfairly.
It is the vaccinated workers who are getting sick with COVID, but it is the unvaccinated who are punished with constant testing, restrictions, and threats of losing their jobs.
The COVID shots are a disaster. Even for the elderly which is supposed to be the most compelling use case, death rates in elderly homes went up by a factor of 5 after the shots rolled out. Each time the shots are given, the deaths spike. Nobody is talking publicly about this. It’s not allowed.
Doctors are seeing rates of injury and death increase dramatically in all ages of people. The injuries are only happening to the vaccinated. There is no doubt that this is happening but many doctors have so much cognitive dissonance that they don’t see it.
One nurse with 23 years of experience says she’s never heard of anyone under 20 dying from cardiac issues until the vaccines rolled out. Now she knows of around 30 deaths.
“I have been a nurse for 36 years. I have NEVER witnessed people in their 20s and 30s having strokes, atrial fibrillation, or cardiomyopathies until the Covid vaccines. I work in cardiology. When I mention that someone should look at the vaccines as a possible reason, I am immediately silenced and told, “It is NOT from the vaccine.””
Doctors aren’t recording vaccination status in the medical records so that all the deaths are attributed to the unvaccinated.
Doctors are deliberately ignoring the possibility that the vaccines could be the cause of all the elevated events. The events are simply all unexplained.
Many doctors have either quit or will quit.
Some doctors and nurses at top institutions such as Mass General Hospital have falsified vaccine cards. They publicly toe the line and encourage their patients to take the shot knowing full well it is deadly. They value their job more than the lives of their patients. The important thing is they are risking 10 years in jail for doing this. These highly respected medical workers are telling the world that these COVID shots are so dangerous that they are willing to risk 10 years in prison to avoid taking the shot. That’s the message America needs to hear. And if Biden were an honest President, he would call for full amnesty and protection from retaliation for all these cases if people admitted publicly they did this. He’d be amazed at the number of responses he’d get. But he won’t do that because it would be too embarrassing for his administration.
Recently a person claiming to represent 'Covid Science' did a sleight-of-hand hack job on my Cancer tracking chart that I derive from CDC data.
We take you through that parade of deception & incompetence in 5 panels, after exemplifying how this work is professionally done below.
The 1st sleight-of-hand he used involves decrementing UCoD depressed cancer deaths from the totals.
He failed to us the Wonder Database to double-check and see if the lowered Cancer death rates were real, or merely an Underlying Cause of Death effect (i.e. Died 'with' Covid).
During the SARS2 coronavirus pandemic, fundamental principles of public health were ignored, and trust in public health has been damaged. As experts in public health, medical science, ethics, and health policy, we propose the following ten principles to guide public health officials and scientists, in order to ensure the credibility of public health recommendations and to help restore public trust.
Ethical Principles of Public Health
1. All public health advice should consider the impact on overall health, rather than solely be concerned with a single disease. It should always consider both benefits and harms from public health measures and weigh short-term gains against long-term harms.
2. Public health is about everyone. Any public health policy must first and foremost protect society’s most vulnerable, including children, low-income families, persons with disabilities and the elderly. It should never shift the burden of disease from the affluent to the less affluent.
3. Public health advice should be adapted to the needs of each population, within cultural, religious, geographic, and other contexts.
4. Public health is about comparative risk evaluations, risk reduction, and reducing uncertainties using the best available evidence, since risk usually cannot be entirely eliminated.
5. Public health requires public trust. Public health recommendations should present facts as the basis for guidance, and never employ fear or shame to sway or manipulate the public.
6. Medical interventions should not be forced or coerced upon a population, but rather should be voluntary and based on informed consent. Public health officials are advisors, not rule setters, and provide information and resources for individuals to make informed decisions.
7. Public health authorities must be honest and transparent, both with what is known and what is not known. Advice should be evidence-based and explained by data, and authorities must acknowledge errors or changes in advice as soon as they are made aware of them.
8. Public health scientists and practitioners should avoid conflicts-of-interest, and any unavoidable conflicts-of-interest must be clearly stated.
9. In public health, open civilized debate is profoundly important. It is unacceptable for public health professionals to censor, silence or intimidate members of the public or other public health scientists or practitioners.
10. It is critical for public health scientists and practitioners to always listen to the public, who are living the public health consequences of public health decisions, and to adapt appropriately.
However, it also shows something much larger: Confirmation that the vaccines have no (mortality) efficacy. That’s what I’ll make clear in this article. The results also point to my recent observation that all of the U.S. statistics appear to be confounded by wealth effects for which no agencies are making statistical corrections.