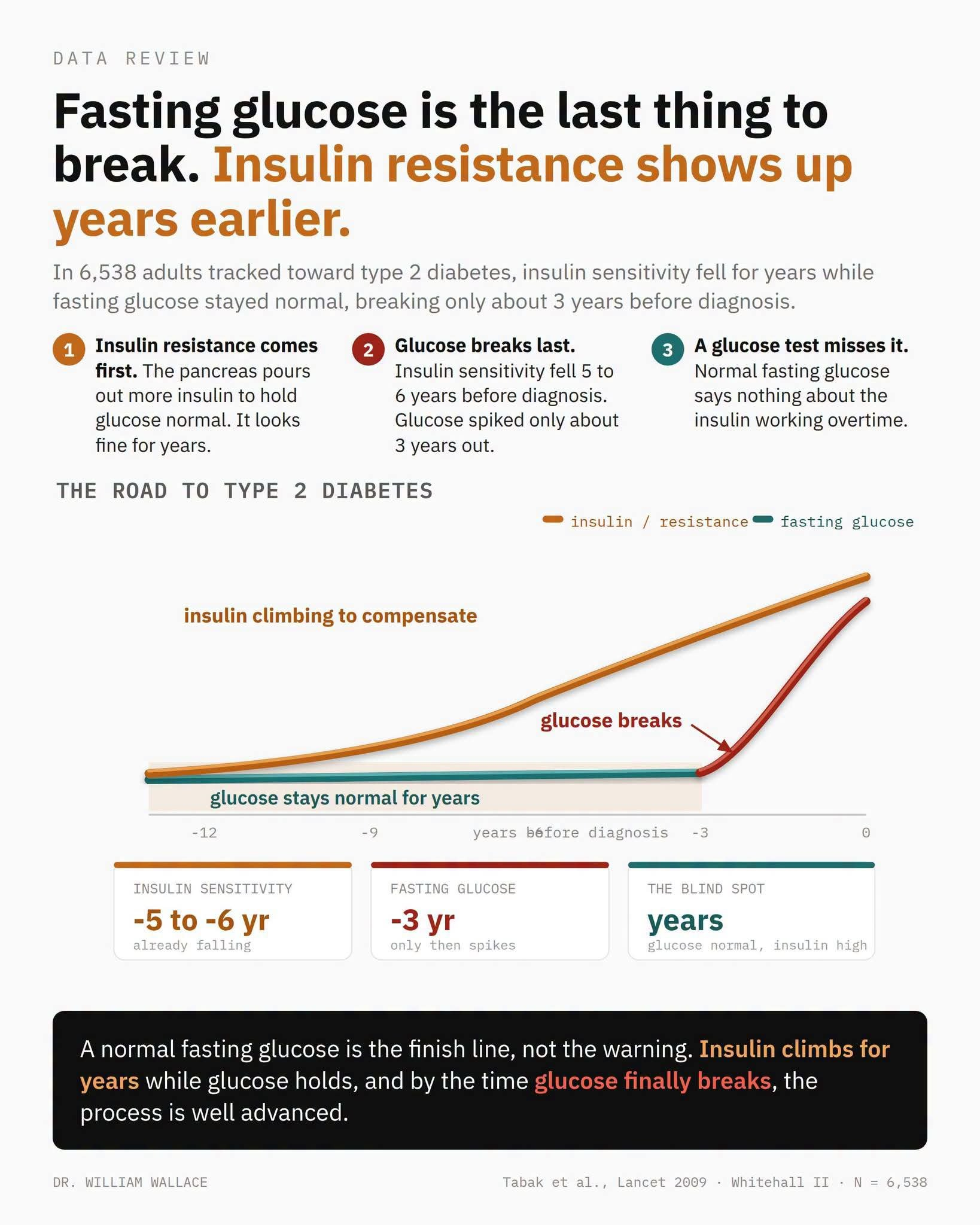
In the Whitehall II study, 6,538 adults without diabetes were tracked for years, and the researchers reconstructed the path of those who developed type 2 diabetes up to 13 years before diagnosis. Insulin sensitivity fell steeply over the five years before diagnosis. Fasting glucose stayed flat and only began its sharp climb about three years out, rising from 5.79 to 7.40 mmol/L. Beta-cell function actually rose first, the pancreas compensating, then collapsed as diagnosis closed in.
Glucose reads normal for years because insulin is quietly working overtime to hold it there. As tissues resist insulin, the pancreas pumps out more to keep the line. Fasting glucose is a lagging indicator: it only moves once the beta cells can’t keep up. Fasting insulin, or HOMA-IR, captures the compensation phase a glucose test misses entirely. By the time glucose crosses the diabetic threshold, the machinery has been straining for years.
Whitehall II was 71% male and 91% white, an occupational cohort, and the pattern can run faster in other populations, as the companion South Asian analysis showed. It’s observational, mapping natural history, not proof that measuring insulin earlier changes anything. Fasting insulin assays aren’t standardized, part of why it isn’t a routine test, and HOMA-IR is a surrogate, not a gold-standard clamp.
insulin resistance is measurable years before fasting glucose moves, so a normal glucose says little about the insulin behind it, and fasting insulin opens a much longer runway to catch dysglycemia early. However, that fasting insulin is a validated screening test with agreed cutoffs, or that acting on it sooner improves hard outcomes. The open question is whether routine fasting-insulin screening plus early intervention lowers diabetes incidence. That trial hasn’t been run.