Everyone is reading the Supreme Court’s Roundup decision as a fight about glyphosate. Much of MAHA called it a betrayal. The more I studied the opinion, the more I concluded it is not really about glyphosate at all.
The justices did not weigh epidemiology. They did not rule on whether glyphosate causes cancer. They did not pick IARC or EPA as the better science. They answered a narrow legal question with enormous consequences.
The question: when EPA approves a pesticide label under FIFRA, can a state jury later decide the manufacturer should have warned more strongly? The Court’s answer was largely no. EPA-approved labels now preempt most state failure-to-warn claims.
Why does that reach beyond Roundup? State failure-to-warn lawsuits have been one of the few mechanisms that surface emerging risk. Tobacco. Asbestos. Lead paint. PFAS. Discovery forced disclosure. Experts testified under oath. Regulators defended their conclusions in open court.
That pathway just narrowed dramatically. When an EPA label preempts the claim, EPA becomes the gatekeeper for deciding when evolving science justifies a new warning. That authority no longer rests with juries hearing new evidence. It rests with one federal agency.
So here is the real question, and it is a constitutional one: Can Congress create a system in which a single federal agency becomes the exclusive gatekeeper for whether evolving scientific evidence ever reaches an American jury?
This is hard to square with two decisions constitutional conservatives celebrated. Dobbs returned power to the states. Loper Bright said courts, not agencies, interpret statutes. Here, an agency’s determination became the basis for closing the courthouse door.
Note who stood where. The Biden administration did not embrace the broad preemption argument. The Trump administration did. Ironically, the Biden position sat closer to conservative legal principles: preserve juries, respect state common law, do not expand the administrative state.
The decision assumes EPA will revisit labels as science evolves. Look at the record. Glyphosate entered review in 2009. EPA reaffirmed “not likely carcinogenic” in 2020. The Ninth Circuit faulted that analysis. EPA withdrew it. More than fifteen years in, still no final determination.
Meanwhile the science moved past cancer. Researchers are now studying endocrine disruption, the gut microbiome, metabolic disease, reproductive and developmental toxicity, neuroinflammation, and cumulative exposure to many chemicals at once. The questions themselves have changed.
Freeze the courts to EPA’s pace and you freeze more than yesterday’s conclusions. You freeze yesterday’s understanding of which questions even deserve investigation. That is a dangerous place for science and for public health.
One more point. If EPA’s science now forecloses jury claims, EPA’s independence is no longer just a regulatory issue. It is a civil-justice issue. The FDA has faced years of scrutiny over capture and the revolving door. EPA has largely escaped it. This decision should end that.
This case is not really about glyphosate. It is about who decides when science has changed, and whether Americans keep access to the courts when new evidence emerges.
In a nutshell, the court’s decision puts all power to regulate (more than just) glyphosate in one agency — the EPA. This obviously risks the EPA becoming yet another captured agency. ABN
The covid mRNA vax appears to have been a well-planned and executed biowarfare attack on Western civilization. Many today still can’t see it. Some are still taking the boosters (17.5% in USA). Repeated boosters contradict elementary vaccinology as they harm the immune system by turning off natural immunity while also training adaptive immunity to ignore the covid virus. This explains both the rise in cancers and other maladies and repeat bouts of covid itself. The covid vax plus covid itself show how huge populations can be manipulated and controlled through words, images, fake science, and emotion. ABN
As DMSO’s therapeutic properties address the root causes of a wide range of diseases, in addition to them alleviating challenging neurological disorders, they also address many challenging disorders of the reproductive tract faced by both men and women, that, once again, medicine consistently falls short in addressing, and since publishing this series, I’ve received an astonishing number of stories from readers whose issues resolved thanks to DMSO which match what’s reported in the literature (e.g., infertility, menstrual issues including cramps or longstanding complications from childbirth). Recently, I finished compiling all of the studies and reader reports (that can be read here), which shows DMSO heals:
•Prostate issues such as BPH (which many readers reported improving), prostate stones, prostatitis (including many cases that did not respond to conventional therapies), and prostate cancer—particularly when used in conjunction with another off-patent therapy (along with mitigating complications from cancer).
•Testicular injuries (e.g., protecting them from radiation or blood loss due to torsions), epididymitis improving fertility (and providing a means to create a safe reversible male birth control) and scrotal injuries.
•Erectile dysfunction, genital infections (e.g., warts or herpes), Peyronie’s disease, priapisms (blood stuck in the penis producing erections over 4 hours, which, after 24 hours often permanently damage the penis), pelvic floor dysfunction, and sexual dysfunction resulting from other genitourinary issues (e.g., prostatitis).
Very good overview of the biolab info released by Gabbard and its global ramifications through covid, covid totalitarian policies, the Ukraine War and more. Since the Gabbard declassification story has been missing in most press outlets, this video is especially well worth watching. I admire and greatly enjoy the brevity and conciseness of the Promethean videos. There are exceptions to this rule, but it applies here — when you really know a subject well, you can describe it clearly and with few words. ABN
For over four decades, the prevailing narrative surrounding AIDS has centered on the HIV virus as its primary cause, as posited by governments and health organizations worldwide. Despite this consensus, alternative theories have been largely suppressed or marginalized. In his book *The Real Anthony Fauci*, Robert Kennedy Jr. highlights the extensive body of evidence supporting these dissenting views, including over 900 references to academic literature. While some praise this work, critics argue that the endorsements come from lesser-known figures in the scientific community. One notable exception is the late Luc Montagnier, the Nobel Prize-winning researcher credited with discovering HIV, who acknowledged the presence of “many untruths” in the mainstream narrative about AIDS and supported Kennedy’s claims, suggesting that the understanding of AIDS and its causes is more complex than originally thought.
Montagnier’s own perspectives on the relationship between HIV and AIDS have evolved over time. In a 1992 interview, he indicated that HIV infection did not necessarily lead to AIDS and that other factors might contribute to the disease’s development. This sentiment echoes the views of other dissident scientists, such as Professor Peter Duesberg, who argued that recreational drug use was a significant factor in the early AIDS cases, rather than HIV itself. Duesberg’s critiques prompted significant backlash from the scientific community, which maintained a strong consensus on the HIV/AIDS connection. The UK’s Chief Medical Officer and other health authorities condemned dissenting views as potentially dangerous misinformation, reinforcing the prevailing narrative that linked HIV infection directly to AIDS.
One of the most significant challenges to the HIV/AIDS paradigm emerged from a 1993 paper published in *Bio/Technology*, which argued that the HIV tests used for diagnosis were never scientifically validated. This paper suggested that the antibodies detected in patients could be due to immune system abnormalities rather than the presence of HIV. The authors contended that the tests were based on circular reasoning, as they were designed to react with antibodies in AIDS patients without proving that these antibodies were specific to HIV. This argument revealed a critical flaw in the scientific basis for HIV testing and the resultant diagnosis of AIDS, casting doubt on the validity of the entire HIV/AIDS narrative.
Despite the overwhelming financial and political investments in the HIV/AIDS model, various researchers, including the Perth group led by Eleni Papadopulos-Eleopulos, have continued to challenge the established view. Their work identified five key mistakes in the foundational science, including the misinterpretation of reverse transcriptase activity and the failure to isolate and purify HIV particles. Additionally, they argued that the correlation between HIV and AIDS is artificial, stemming from the nature of the tests rather than a clear causal relationship. Their findings suggest that lifestyle factors, such as drug use and certain sexual practices, may be more relevant to the observed health crises than the presence of a virus. Despite decades of criticism and censorship, the critiques and alternative explanations offered by these researchers call for a reevaluation of the HIV/AIDS framework and its implications for public health and treatment strategies, potentially benefiting millions in the process.
The above is an AI summary offered by the website which has posted the full article. The summary is a convenience for interested readers. Coincidentally, to my knowledge, Fauci is widely believed to have had as large a role in the ‘HIV myth’ as he has had in the covid-19 scamdemic. It is possible Fauci will be revealed to be the most successful psychopathic medical murderer in world history. ABN
Over 70% of humanity underwent a chemical lobotomy masquerading as “vaccination.” This explains the widespread collapse of common sense, deterioration of cognitive function, and drastic personality distortions seen since 2021. Safety signals identified in our two peer-reviewed studies include:
PRION DISEASE — 847× more likely vs. flu shot
BRAIN CLOTS — 3,000× more likely
PSYCHOSIS — 440× more likely
HOMICIDAL IDEATION — 25× more likely
DEMENTIA — 140× more likely
SUICIDAL THOUGHTS — 150× more likely
SCHIZOPHRENIA — 315× more likely
DEPRESSION — 530× more likely
HERPES ZOSTER MENINGITIS — 1,200× more likely
TOXIC ENCEPHALOPATHY — 157× more likely
MENINGITIS (ALL TYPES) — 34× more likely
AUTOIMMUNE ENCEPHALITIS — 79× more likely
BRAIN ABSCESS — 120× more likely
SPINAL CORD ABSCESS — 89× more likely
VIOLENT BEHAVIOR — 80× more likely
COGNITIVE DECLINE — 115× more likely
DELUSIONS — 50× more likely
MYELITIS (ALL TYPES) — 31× more likely And many more…… The mRNA shots disrupt the blood–brain barrier, allowing mRNA, amyloidogenic spike proteins, and pathogens to penetrate the brain and spinal cord — an outcome consistent with the skyrocketing rates of cognitive decline now seen across the world.
__________
I am seeing fairly widespread vax injury among people I know, and whom I know about through friends. It sounds so bad it’s hard to believe. But just as many people can enter early, and later stages of, dementia with little or no realization of what is happening, drug or surgically induced brain injuries can be inflicted without sufferers realizing that anything has happened to them at all. Mind-control poisons work in this way. They can be administered slowly (repeated shots or covert doses); or quickly as, in some cases, the type of drug or procedure, like lobotomy, may not be recognized by victims even though much of their intrinsic behavior has changed greatly. Rather than understand that they have been attacked, such victims may decide they are just getting old or losing it for some other reason, like a recent accident or drinking bout. Many people in the West have succumbed to weakened vitality and motivation due to clandestine poisoning and maiming by enemies of the West who are living among us and who often pose as friends. This explains the remarkably anemic response the West is evincing as it is slowly being methodically annihilated. ABN
A single dose of psilocybin, a psychedelic that acutely causes distortions of space–time perception and ego dissolution, produces rapid and persistent therapeutic effects in human clinical trials1,2,3,4. In animal models, psilocybin induces neuroplasticity in cortex and hippocampus5,6,7,8. It remains unclear how human brain network changes relate to subjective and lasting effects of psychedelics. Here we tracked individual-specific brain changes with longitudinal precision functional mapping (roughly 18 magnetic resonance imaging visits per participant). Healthy adults were tracked before, during and for 3 weeks after high-dose psilocybin (25 mg) and methylphenidate (40 mg), and brought back for an additional psilocybin dose 6–12 months later. Psilocybin massively disrupted functional connectivity (FC) in cortex and subcortex, acutely causing more than threefold greater change than methylphenidate. These FC changes were driven by brain desynchronization across spatial scales (areal, global), which dissolved network distinctions by reducing correlations within and anticorrelations between networks. Psilocybin-driven FC changes were strongest in the default mode network, which is connected to the anterior hippocampus and is thought to create our sense of space, time and self. Individual differences in FC changes were strongly linked to the subjective psychedelic experience. Performing a perceptual task reduced psilocybin-driven FC changes. Psilocybin caused persistent decrease in FC between the anterior hippocampus and default mode network, lasting for weeks. Persistent reduction of hippocampal-default mode network connectivity may represent a neuroanatomical and mechanistic correlate of the proplasticity and therapeutic effects of psychedelics.
It is my understanding that the Buddha and/or the Buddhist tradition was and always has been well aware of psilocybin and probably other psychedelics and herbal drugs, like opium and cannabis.
In light of this, it is significant that the Fifth Precept for lay Buddhists proscribes only alcohol, and it does this very specifically by mentioning two types of alcoholic beverages (fermented and distilled) and nothing else. The Fifth Precept does not mention any other drugs.
As modern Buddhists, we can see that this conforms with what many of us have experienced with psychedelics and cannabis, among other ‘recreational’ drugs. Of course those drugs can be harmful but they can also do people a lot of good. Alcohol use, on the other hand, too often leads to very dangerous and spiritually stultifying mental conditions that do no one any good.
I have no problem with Buddhist teachers extrapolating the meaning of the Fifth Precept to include other drugs and sensory indulgences, but also believe that paying attention to the original meaning and its socio-environmental context (when people knew lots about plants) is important to keep in mind.
Merck & Co. has reached an agreement to pay $50 million to settle hundreds of Gardasil lawsuits, which raise allegations that the controversial HPV vaccine’s side effects left young adults with serious neurological and other adverse health problems.
The Gardasil settlement was reported by Bloomberg News on June 4, indicating that the deal was confirmed in an emailed statement from Merck officials. Following years of litigation, Merck claims that the payouts should resolve all lawsuits over the HPV vaccine, except for one remaining case.
First introduced in 2006, Gardasil is a widely used vaccine administered to young girls and boys for the prevention of human papillomavirus, or HPV, infections, which can cause cervical cancer and other forms of cancer. HPV is sexually transmitted, and the vaccine has been promoted as an important tool for preventing HPV-related cancers later in life.
In 2022, the New England Journal of Medicine published the results of the NordICC trial — the first randomised controlled study of colonoscopy screening ever conducted. Over 84,000 people were followed for ten years. The trial found an 18% reduction in cancer incidence and no significant reduction in cancer deaths. To prevent a single case of colorectal cancer, 455 people had to be invited for screening. To prevent a single death, the numbers were statistically indistinguishable from zero.¹
This is the pattern.
Across the major screening programmes — mammography, PSA, Pap, colonoscopy, lung CT — when the question is whether the screened population actually outlives the unscreened population, the benefit largely disappears.² The statistic the programmes advertise is disease-specific mortality: deaths from the disease the test is looking for. The statistic they bury is all-cause mortality: whether the screened group, taken as a whole, lives longer. The two numbers are not the same. You can reduce deaths from one disease while total deaths remain flat — because treatment has killed as many people as the disease prevented, or because the disease you found was never going to kill anyone.²
The screened do not live longer than the unscreened. They are more likely to spend their remaining years monitored, biopsied, cut, and medicated for conditions that would not have harmed them. This essay catalogues twelve tests that produce that conversion, organised by the four mechanisms through which it is achieved.
Test time has arrived: the first person has been treated in a highly anticipated gene-therapy trial that aims to coax aged cells to take on a younger identity.
The clinical trial is testing an innovative technique that involves turning on three genes that can ‘partially reprogram’ old cells, allowing them to behave as if they were young again. Some scientists argue that partial reprogramming could rejuvenate old organs. But this trial will test the activation of these three genes as an approach for treating disease — in this case, a form of glaucoma, a condition that can cause blindness.
The hope is that the proteins encoded by the genes will enable regeneration of neurons in the optic nerve, which connects the eye to the brain and is damaged in people with glaucoma. These neurons are not normally capable of regeneration. The company sponsoring the trial, Life Biosciences in Boston, Massachusetts, announced today that it had treated its first participant.
…While dementia, which affects 7 million Americans, worsens over time, doctors in Brazil, where the woman lives, sought to find out if the hallucinogen psilocybin – found in ‘magic mushrooms’ – could stall her decline.
Doctors writing in a medical journal said the woman was given 5g of psilocybin – a large dose sometimes nicknamed a ‘heroic dose’ – in a supervised session, which triggered profuse sweating and a drop in body temperature before she entered a long sleep-like state.
But after about 19 hours, the woman began having conversations on her own, which lasted several hours.
Over the next few days, she was also able to control her bladder, dress and walk by herself and hold eye contact and smile at her loved ones.
A month later, the woman was given a second 3g dose of psilocybin. Instead of falling asleep, she was reportedly conversational and expressive the whole time, describing emotional scenes like surfing with her son on a peaceful island.
The woman also spontaneously told her healthcare team, ‘It is pleasant to come here.’
‘Facial expressivity, emotional reciprocity, spontaneous humor, and gait agility appeared markedly improved,’ doctors from the University of Sao Paulo in Brazil wrote in the journal Frontiers in Neuroscience.
There were no adverse effects, which can include agitation and cardiovascular instability, such as a high heart rate or blood pressure.
The Nuremberg Code of ethics is laudable, but the trials themselves today appear dubious at best and a travesty of justice at worst. I mention this because of the video’s title, and also because it should be mentioned frequently enough to remind us that history, too, is highly susceptible to fraudulent revisions which support deeply impactful falsehoods in the present. The entire downfall of the West today is largely explainable by historical lies which have inculcated the vast majority of Westerners with self-destructive ideas of who they are and what they can become. Covid itself was a lie as are its dominant prescribed treatments, or prescribed lack thereof. ABN
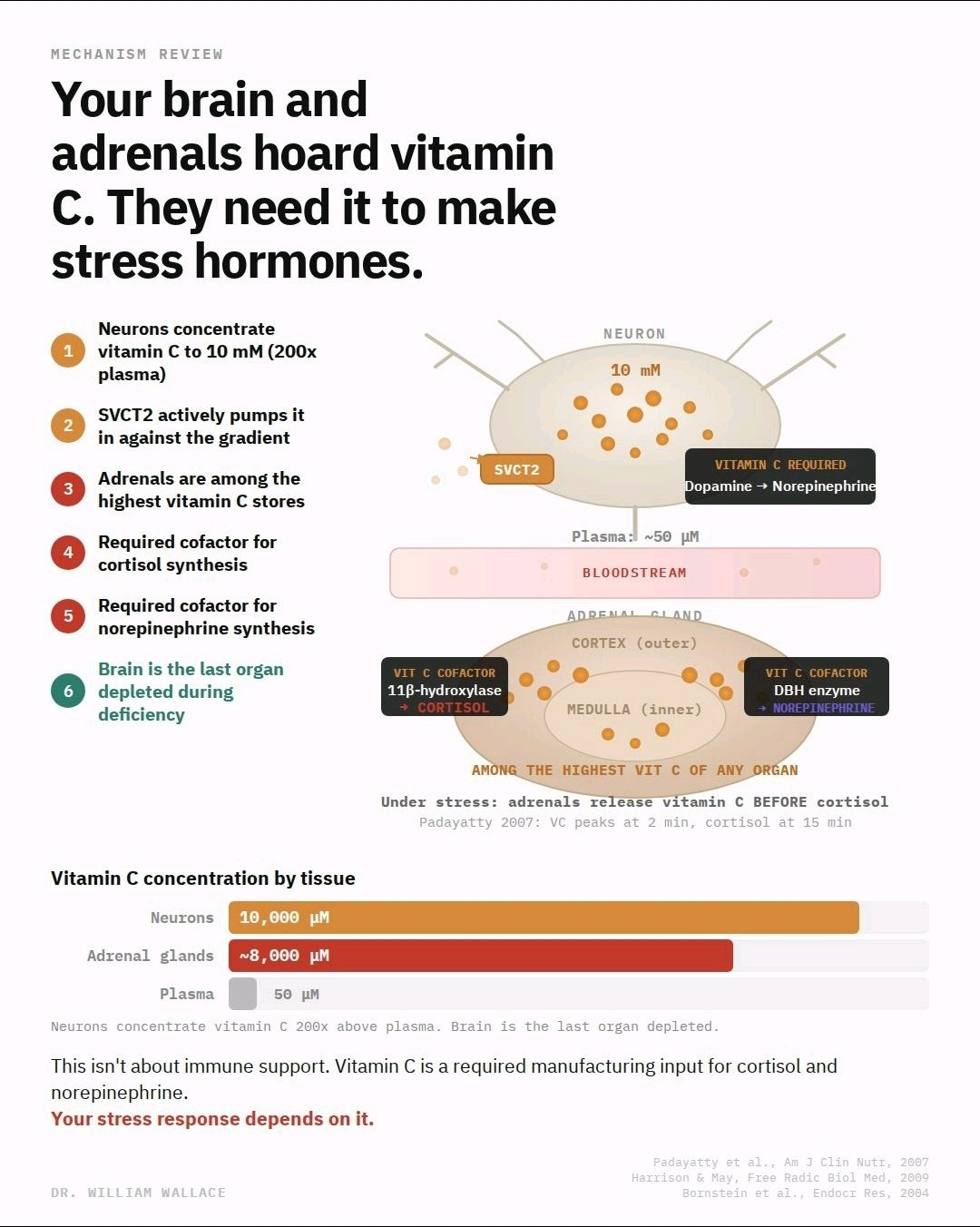
Neurons accumulate vitamin C to approximately 10 mM intracellularly, roughly 200 times the concentration found in plasma. This gradient is maintained by SVCT2, a sodium-dependent transporter expressed almost exclusively in neurons in vivo. The brain is also the last organ to be depleted during deficiency. In guinea pigs (which, like humans, cannot synthesize vitamin C), the brain retained 24% of its vitamin C stores after 14 days of zero intake, while the adrenal glands dropped to 4% and the spleen to 3%. The body prioritizes the brain above everything else.
The adrenal glands are the other major site of accumulation. Vitamin C is a required cofactor for two enzymes central to the stress response: 11β-hydroxylase, which catalyzes the final step of cortisol synthesis in the adrenal cortex, and dopamine β-hydroxylase, which converts dopamine to norepinephrine in the adrenal medulla.
Padayatty et al. (2007) measured this directly in 26 human patients. After ACTH administration, adrenal vein vitamin C concentration surged from 39 to 162 μmol/L within 2 minutes, while cortisol did not peak until 15 minutes. The adrenals released vitamin C before they released cortisol. This sequence suggests ascorbate must be mobilized for steroidogenesis to proceed.
This doesn’t mean mega-dosing vitamin C will improve your stress response. Most of this work describes what happens during deficiency or acute demand, not supplementation above adequate intake. But it does reframe what vitamin C actually does in your body: it’s not primarily an antioxidant or immune molecule. It’s a required manufacturing input for cortisol and catecholamines, concentrated exactly where those hormones are made.
Harrison & May, Free Radic Biol Med, 2009. Padayatty et al., Am J Clin Nutr, 2007. Bornstein et al., Endocrine Research, 2004.