Back in July 2021, many scientists had the ill-founded view that the C-19 pandemic was dying out and entering an endemic state. Based on my understanding of the interplay between the virus and the immune system, I knew that this was not going to be the case and reacted immediately to this misinterpretation (https://www.voiceforscienceandsolidarity.org/scientific-blog/a-last-word-of-caution-to-all-those-pretending-the-covid-19-pandemic-is-toning-down). Once again, many scientists find themselves with the belief that the emergence of the Omicron variant announces the end of the pandemic and the virus’ transition into endemicity. Their prediction is largely based upon the initial observation that Omicron seems to be causing rather mild disease symptoms which they interpret as being indicative of a virus that—although more infectious—is now becoming less virulent and, therefore, increasingly featuring endemic behavior. I am afraid that once again, I don’t agree—a pandemic can only be tamed by herd immunity. Given the high vaccine coverage rates in most industrialized countries, we have generated anything but herd immunity. I also have yet to hear any compelling evidence concerning significant mutations in the genes that determine SARS-CoV-2’s virulence. Perhaps we should think twice before making statements that are not supported by immunological evidence.
The importance of understanding SARS-CoV-2 evolution cannot be overlooked. Recent studies confirm that natural selection is the dominating mechanism of SARS-CoV-2 evolution, which favors mutations that strengthen viral infectivity. Here, we demonstrate that vaccine-breakthrough or antibody-resistant mutations provide a new mechanism of viral evolution. Specifically, vaccine-resistant mutation Y449S in the spike (S) protein receptor-binding domain, which occurred in co-mutations Y449S and N501Y, has reduced infectivity compared to that of the original SARS-CoV-2 but can disrupt existing antibodies that neutralize the virus. By tracking the evolutionary trajectories of vaccine-resistant mutations in more than 2.2 million SARS-CoV-2 genomes, we reveal that the occurrence and frequency of vaccine-resistant mutations correlate strongly with the vaccination rates in Europe and America. We anticipate that as a complementary transmission pathway, vaccine-breakthrough or antibody-resistant mutations, like those in Omicron, will become a dominating mechanism of SARS-CoV-2 evolution when most of the world’s population is either vaccinated or infected. Our study sheds light on SARS-CoV-2 evolution and transmission and enables the design of the next-generation mutation-proof vaccines and antibody drugs.
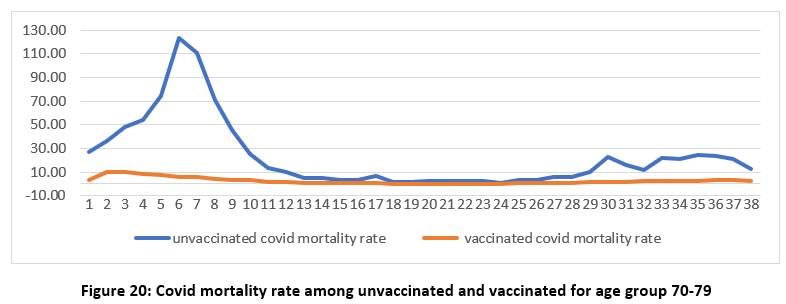
1.Our research team have now analysed the ONS England November mortality data. We conclude that despite seeming evidence to support vaccine effectiveness this conclusion is doubtful because of a range of serious inconsistencies and anomalies.
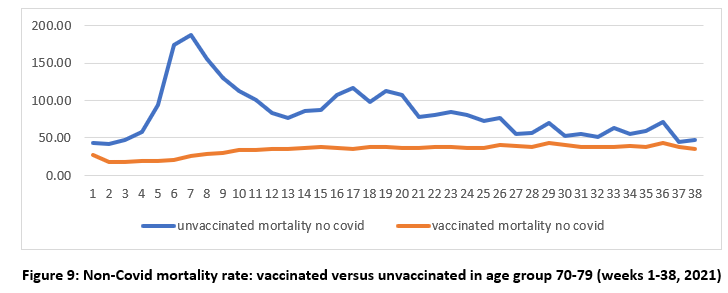
2.The data appear to show lower non-Covid mortality for the vaccinated compared to the unvaccinated. Odd. Also unvaccinated mortality rates peak at the same time as the vaccine rollout peaks for the age group, then falls and closes in on the vaccinated. This is not natural
3. Consider what we are witnessing here. We have a vaccine whose recipients are suffering fewer non-covid deaths and hence are benefitting from improved mortality. And the mortality rates look to differ significantly from historical norms, as evidenced in mortality lifetables.
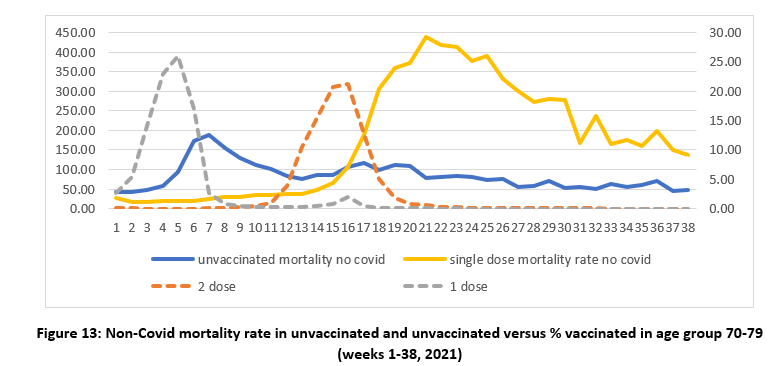
4.Correlating unvaccinated mortality with vaccine roll out we see curious patterns (dotted line the proportion of people getting first and second doses). Why are the unvaccinated dying after NOT getting the 1st dose? Why are the single dosed dying after NOT getting the 2nd dose?
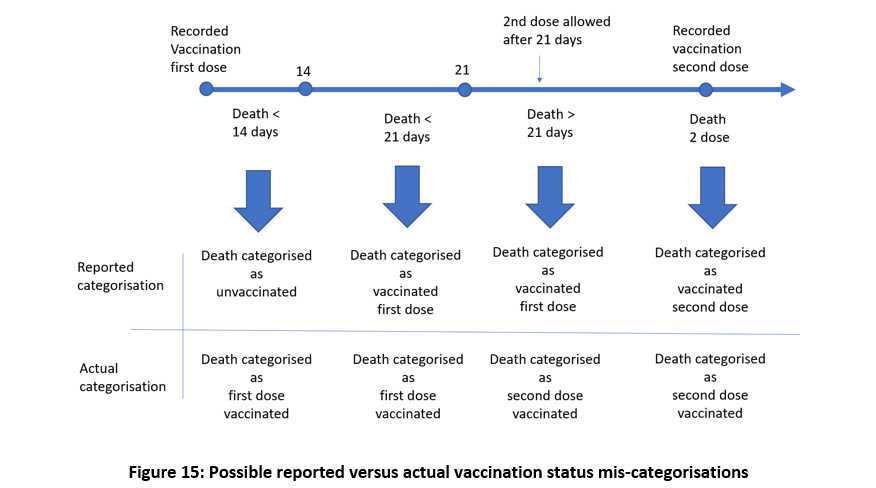
5.Plenty of evidence that the vaccinated who die within 14 days of vaccination may be categorized as unvaccinated. Then someone who dies within 14 days of first dose is miscategorised as unvaccinated and a similar thing could occur post second dose.
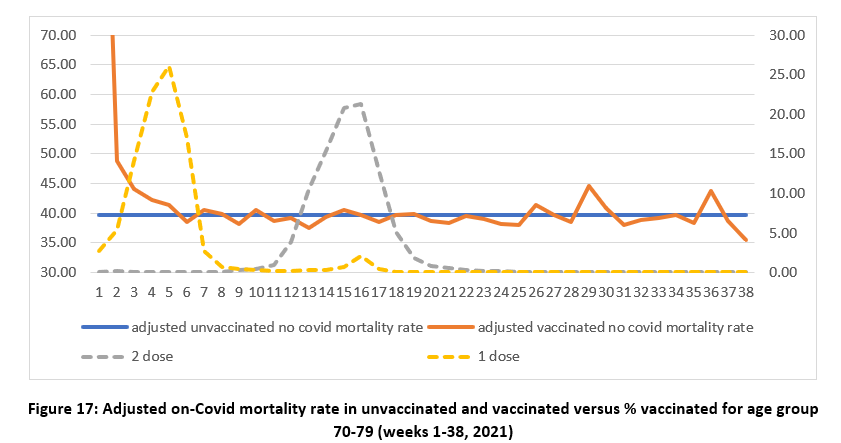
6. Miscategorization might explain odd phenomena in ONS mortality. To correct the error we can take the difference between the expected mortality for the unvaccinated and the data, and re-allocate this unexpected excess mortality to the vaccinated to get new ADJUSTED estimates.
7. The early spikes in mortality that appear to occur soon after vaccination may be caused by the infirm, moribund, and severely ill receiving vaccination in priority order and thus simply appearing to hasten deaths that might otherwise have occurred later in the year.
8.Turning to Covid mortality, at face value, there appears to be clear evidence of vaccine effectiveness. But……..
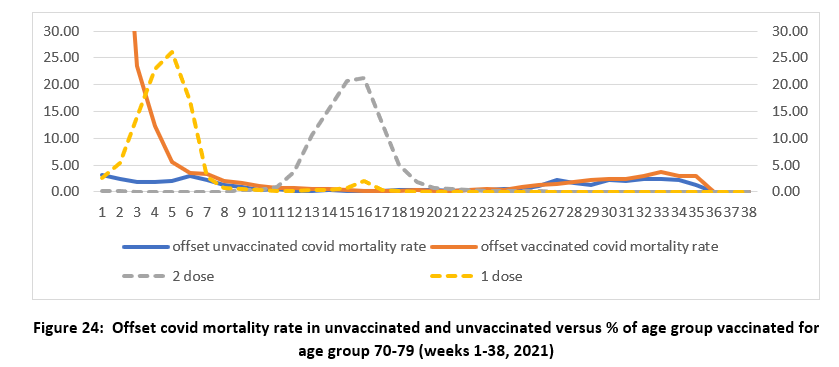
9.After vaccination people endure weakened immune response for a period of up to 28 days and may be in danger of infection from Covid or other infectious agent at any time in that period. It therefore makes sense to examine infection date rather than date of death registration.
10.We adjust for this using a temporal offset and see a large spike in mortality for all age groups during the early weeks, when covid prevalence was high, and when the first dose vaccination rollout peaked.
11.After our offset adjustment we observe no significant benefit of the vaccines in the short term. They appear to expose people to an increased mortality, in line with what we know about immune exposure or pre-infection risks,
12.Whatever the explanations for the observed data, it is clear that the ONS data is both unreliable and misleading. Absent any better explanation Occam’s razor would support our conclusions. The ONS data provide no reliable evidence that the vaccines reduce all-cause mortality.
This is the latest of numerous attempt to decode ONS hieroglyphs, but now we may have stumbled upon a rosetta stone to help solve the puzzle.
Strong data from a peer reviewed article in the journal of Clinical Infectious Disease shows that there is a significant increase in the risk of myocarditis/pericarditis following Comirnaty vaccination among Chinese male adolescents, especially after the second dose. Onset of myocarditis was a median of 2 days after vaccination. The clinically significant (acute and/or “mild”) myocarditis/pericarditis incidence rate came in at one out of every 2680 young males.
There has been a significant rise in new SARS-CoV-2 infections in the Gauteng Province in the last four weeks which has been attributed to the new Omicron variant announced on 24 November 2021. The first cases of Omicron were detected in the Tshwane District and coincided with the sharp rise in new infections, heralding the onset of the fourth wave in Gauteng.
Tshwane has been the global epicentre of the Omicron Outbreak and the Gauteng Province Fourth Wave with the weekly number of cases rising exponentially over several weeks, reaching just over 8569 cases in Epi Week 47 (21 November – November 27 and 41 921 by 3 December before the end of Epi Week 48 (28 November to 4 December). The exponential rise in cases has continued with 9929 new cases reported in Tshwane in the last 5 days from 29 November to 3 December 2021 (Figure 1).
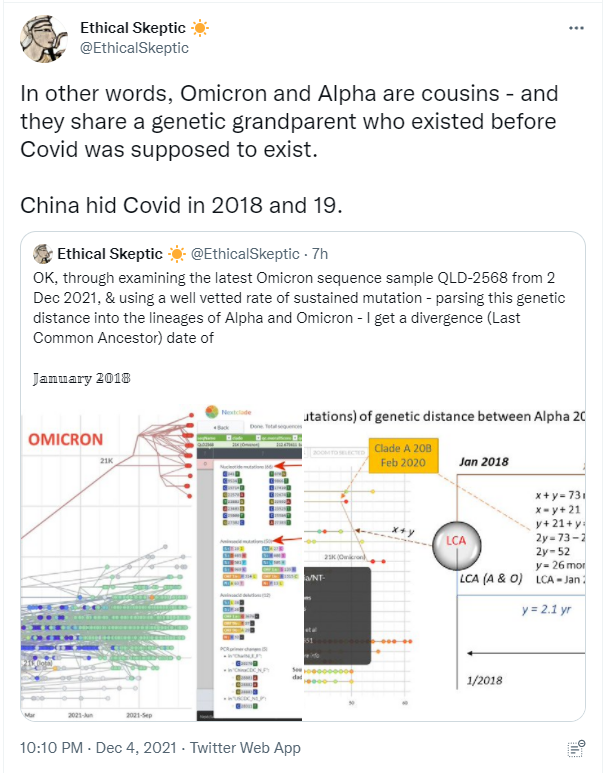
This is probably a very big deal. Omicron or very similar could be the virus China released in 2017 to inoculate its population in preparation for the 2019 deliberate release of covid-19 in Wuhan. There is every reason to assume Western intelligence services knew that a novel respiratory virus was active in East Asia (centered around China) as early as 2017. In another Tweet TES says: “It was not as deadly during those two years [2017-2018]. And it was not hidden completely. Pig Ebola was a good cover story, but intel services hit onto something going on…” With this sort of assumption we can still consider that Western IC knew about the early virus and was well-prepared for the release of a stronger relative in 2019; and thus able to use covid-19 to seize even more power and wealth through our disastrous (for everyone else) “lockstep” covid responses. Other hypotheses are worth considering but this finding does strengthen the one that China released a milder inoculant virus in 2017 in preparation of the stronger covid-19 version. Their aim was most likely to unseat Donald Trump, an aim shared by Western IC and pursued accordingly. It would be reasonable to suspect collusion between China and West in this. ABN
Mandates run counter to the universal medical dictum of risk stratification, whereby treatment is tailored to individuals based on individual risks and benefits to be accrued
The risk/benefit of Covid vaccines is arguably most accurately measured by an all-cause mortality rate comparison of vaccinated against unvaccinated, since it not only avoids most confounders relating to case definition but also fulfils the WHO/CDC definition of “vaccine effectiveness” for mortality. We examine the latest UK ONS vaccine mortality surveillance report which provides the necessary information to monitor this crucial comparison over time. At first glance the ONS data suggest that, in each of the older age groups, all-cause mortality is lower in the vaccinated than the unvaccinated. Despite this apparent evidence to support vaccine effectiveness-at least for the older age groups-on closer inspection of this data, this conclusion is cast into doubt because of a range of fundamental inconsistencies and anomalies in the data. Whatever the explanations for the observed data, it is clear that it is both unreliable and misleading. While socio-demographical and behavioural differences between vaccinated and unvaccinated have been proposed as possible explanations, there is no evidence to support any of these. By Occam’s razor we believe the most likely explanations are systemic miscategorisation of deaths between the different categories of unvaccinated and vaccinated; delayed or non-reporting of vaccinations; systemic underestimation of the proportion of unvaccinated; and/or incorrect population selection for Covid deaths.
Question: Should vaccinated people go get their booster shots or not?
Answer: From an immunological point of view, boosters and mass vaccination in general are as harmful as mold on a wall.
The vaccine can not prevent infection nor transmission. By again increasing the antibodies (with the booster), the virus is put under an even higher immune pressure while further expanding its capacity to escape from the vaccinal antibodies (Abs). As a result more infectious variants gain a competitive advantage and hence, will spread stronger amongst the population.
I am a big fan of Vanden Bossche. He is one of the great fighters on our side. His veterinary background has allowed him to understand how herds respond to diseases and vaccinations and how mass vaccinations can sometimes cause extreme harm to the entire herd, a direction we are steadily moving in right now. Listen as he explains how the covid vaxxes are suppressing immune systems while at the same time pushing the virus to evolve variants that can evade the vaxxes. What he is and has been saying for a year now is not hard to understand. Are our health officials so pig-headed they have never done this basic research yet force mandates anyway? Or is there something more sinister at work? I honestly do wonder. ABN