Tag: medical science
Japanese Surgeon Calls for Suspension of COVID Boosters
In a letter to the peer-reviewed journal Virology, a Japanese cardiovascular surgeon, Dr. Kenji Yamamoto, has called for the discontinuation of COVID-19 booster shots. “As a safety measure, further booster vaccinations should be discontinued,” Yamamoto wrote. Among his urgent concerns are the fact that the COVID-19 vaccines have been linked to vaccine-induced immune thrombotic thrombocytopenia, which, in some cases, has been lethal to patients.
Yamamoto works at Okamura Memorial Hospital in Shizuoka, Japan. In the letter he explains that he and his colleagues have “encountered cases of infections that are difficult to control,” including some that occurred after open-heart surgery and were still not under control after several weeks of treatment with multiple antibiotics.
These patients, says Yamamoto, showed signs of being immunocompromised, and some of them died.
Yamamoto believes their suppressed immune function is likely to have been caused by COVID-19 vaccination.
link
China’s CCP Concealed SARS-CoV-2 Presence in China as Far Back as March 2018
A world inquiring about the origins of SARS-CoV-2 has been met with repeated antipathy and lack of cooperation on the part of the Chinese Communist Party. Consequently, any speculation that the CCP concealed the presence of SARS-CoV-2 prior to December 2019 must be researched through an examination of corroborating yet circumstantial evidence. Inference which may be ascertained only through prosecution along a series of must-answer critical questions.
The Chinese Communist Party owes the entire world restitution for its negligent handling and release of a virus which they fully understood could be deployed as a weapon of war. A virus which has destroyed human rights, worldwide economies, and furthermore resulted in over 5 million deaths globally to date.
link
Note the date of this piece—11/15/21. Ethical Skeptic has consistently provided deeper and better analysis of covid than anyone I know of. The linked essay is still valid. I highly recommend his Twitter account for frequently updated, incisive insights into the history, evolution, and real-world effects of covid. ABN
Dr Peter McCullough: Evidence mounts as government and fake news suppress facts
ISRAEL: Twitter Censors Pfizer-Injured Israeli COVID Vaccine Director
…Last week, Twitter censored Prof. Shapira—who was “physically injured” after his third Pfizer vaccine—and forced him to remove a post which said: “Monkey pox cases were rare for years. During the last years a single case was documented in Israel. It is well established the mRNA vaccines affect the natural immune system. A monkey pox outbreak following massive covid vaccination: *Is not a coincidence.”
link
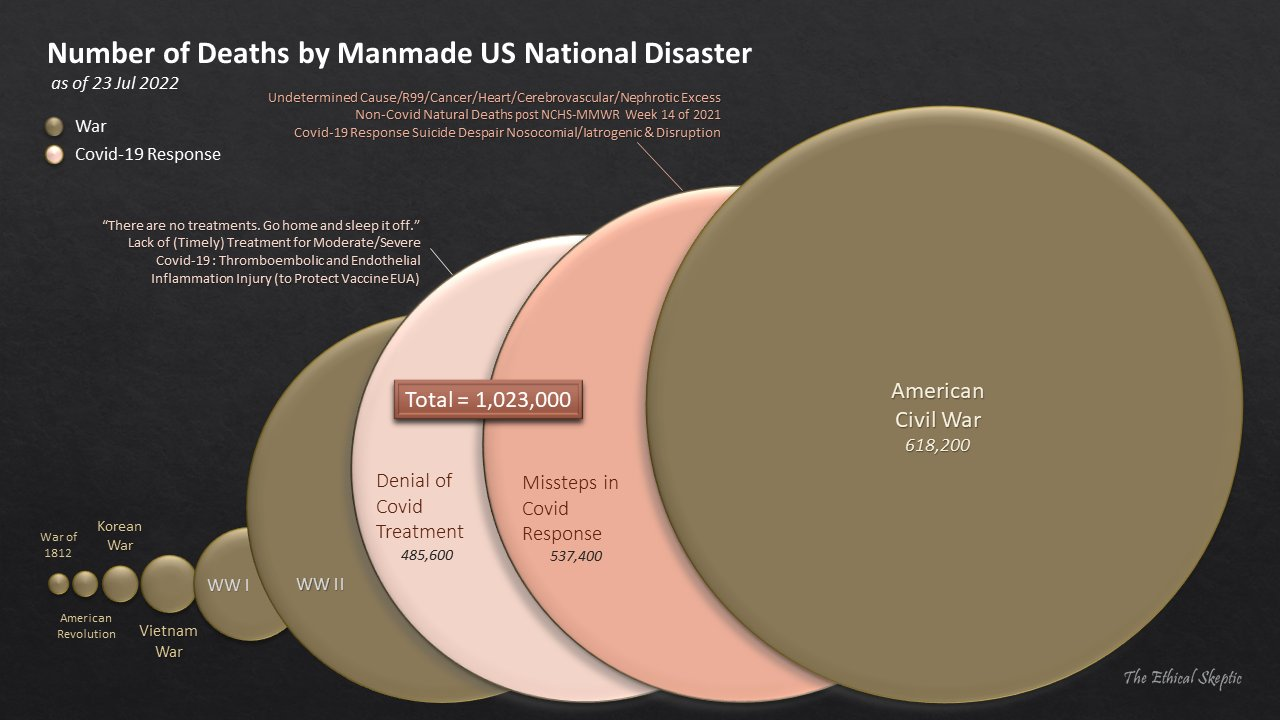
Covid deaths compared to Civil War deaths
Dr. Yan – CCP Weaponising “Red Code” Social Credit Scores Using Children, Monkeypox, and More
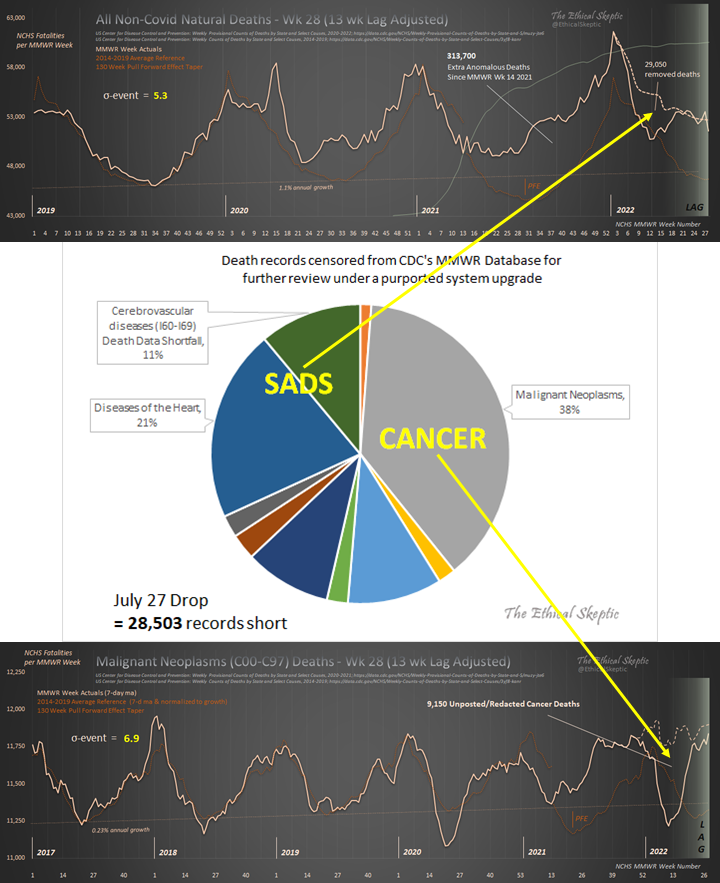
Cancer deaths are way up since mass vaccine rollout
Dismal news from the NCHS MMWR Week 29 drop.
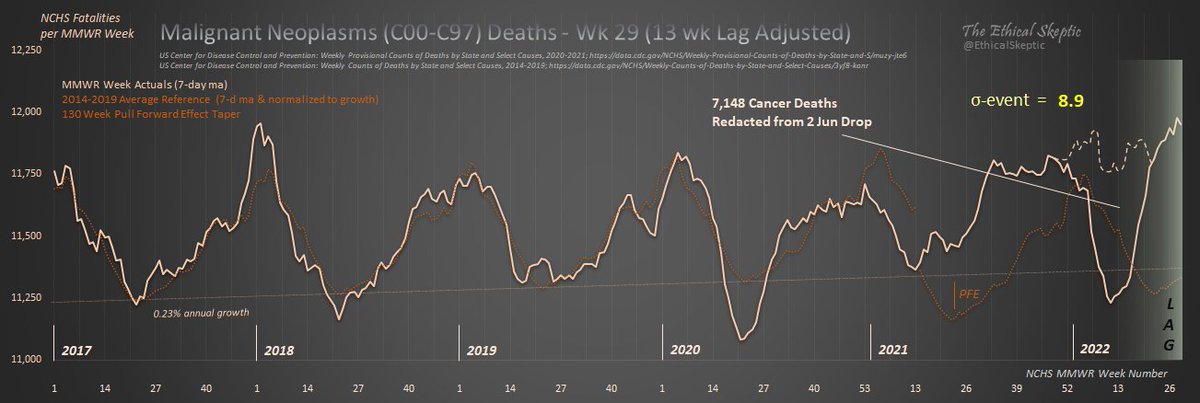
We start with the worst news. I don't like having to see nor show this. Despite the CDC pulling 7,148 records out of cancer deaths (after already posting them on 2 Jun)…
𝗖𝗮𝗻𝗰𝗲𝗿 𝗱𝗲𝗮𝘁𝗵𝘀 𝗮𝗿𝗲 𝗮𝘁 𝟴.𝟵 𝘀𝗶𝗴𝗺𝗮
1⃣
Similarly, Excess Non-Covid Natural Cause Deaths 𝗮𝗿𝗲 𝗮𝘁 𝟲.𝟮 𝘀𝗶𝗴𝗺𝗮 high – despite the 27,829 records pulled from that category from the 2 Jun drop.
Making 331,000 deaths from the unknown factor which arrived MMWR Wk 14 2021.
Continue reading “Cancer deaths are way up since mass vaccine rollout”Robert Malone on government’s “clear and unequivocal decision not to pursue the importance of vitamin D” in preventing covid and flu
I remember a video of Fauci himself maybe 18 months ago saying he takes 6,000 IU Vitamin D daily. But has never advocated for it and many other simple preventatives —zinc, quercetin, magnesium, nasal wash, Vitamin C, etc. ABN
UNDERREPORTING FACTORS FOR VAERS ARE VASTLY UNDERREPORTED
This OpEd will show that the underreporting factors (URFs) for COVID-19 “vaccine”-induced deaths in VAERS have been vastly underreported, resulting in lower numbers of COVID-19 “vaccine”-induced deaths in the total population than have been actually experienced. The OpEd will present the URF computations in the context of a cost-benefit analysis of COVID-19 “vaccines” for the elderly (65+), where costs are the deaths induced by the COVID-19 “vaccines” and benefits are the true COVID-19 deaths that only a COVID-19 “vaccine” could have prevented. The analysis will start with a cost-benefit analysis based on CDC-supplied COVID-19 death numbers and COVID-19 “vaccine” death numbers and then correct for both these CDC-supplied numbers to get real-world cost-benefit results for the COVID-19 “vaccines.” Both the URFs and the cost-benefit ratios are high, even for the 65+ demographic who have highest priority and need for any COVID-19 “vaccine” or treatment.
link
Dose-dependent hospitalizations per million: Australia, NSW
Jaxen with Bigtree, NSW Smalley analysis govt data. Risk of hospitalization dose dependent on number of mandated products. 37 x more likely to be hospitalized. Could be confounded by frailty and other factors, but dose dependency striking new finding C/W immune imprinting.
Originally tweeted by Peter McCullough, MD MPH (@P_McCulloughMD) on August 1, 2022.
Dr Drew and Dr Kelly Victory strongly excoriate covid vaccines: “The ramifications are so profound” they cannot admit it
A scientific scandal with huge implications for women’s health is brewing and you weren’t going to hear about it – until now
TLDR: A paper was published in October showing how the mRNA vaccines could massively impact ovarian and breast cancer risk. Two scientists linked to the NIH and Pharma conspired to remove it from publication – putting a generation of women at risk.
link
“It’s clear now that the vaccines cause fatal myocarditis” – Dr Peter McCullough
BlazeTV with Sara Gonzales. No degree of myocarditis is acceptable as an iatrogenic complication. The cases reported in the literature are serious, long-lasting, and in some reports, fatal. Late gadolinium enhancement is seen on cardiac MRI and has not resolved in some cases.
Originally tweeted by Peter McCullough, MD MPH (@P_McCulloughMD) on July 29, 2022.